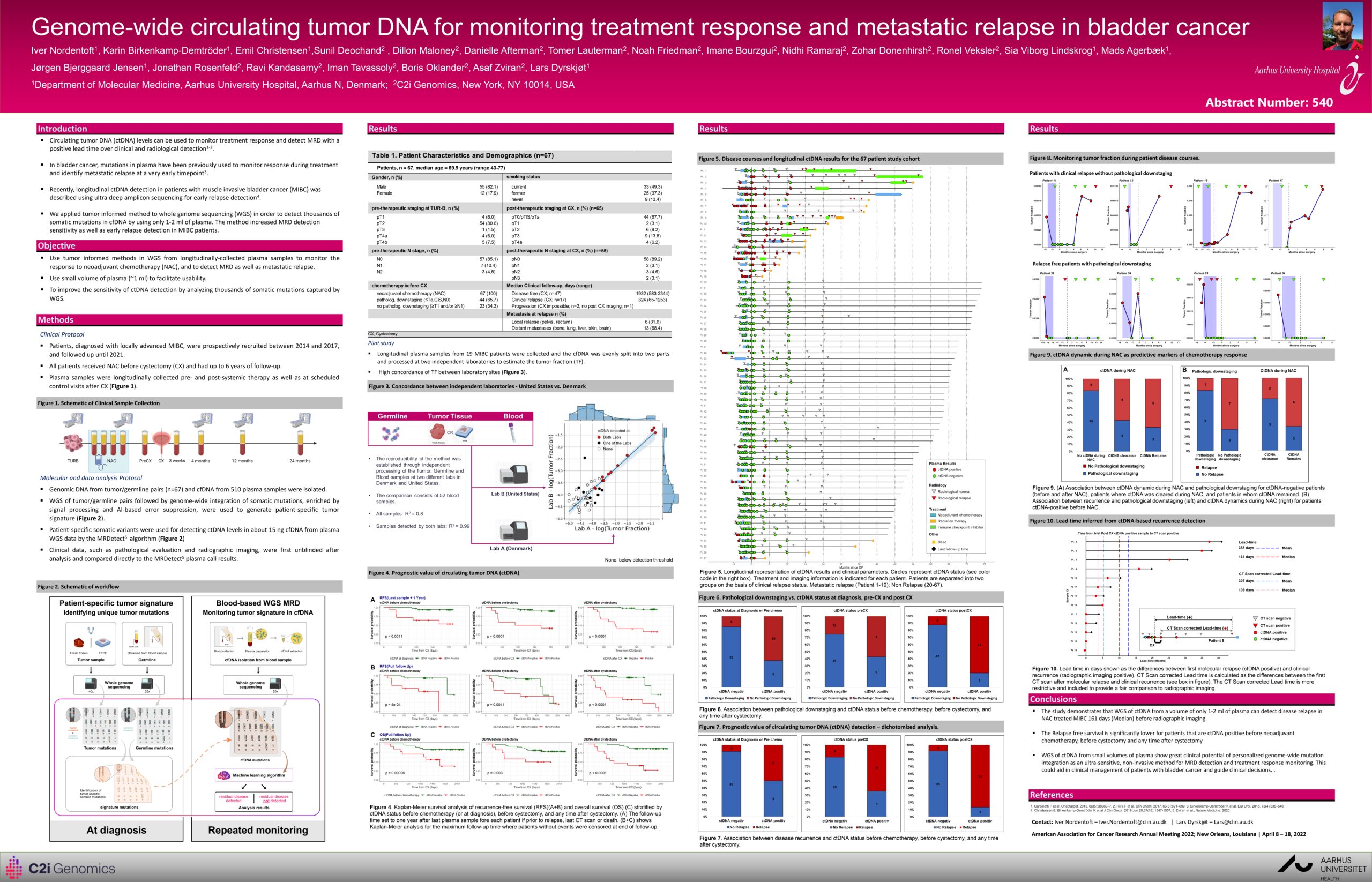
Figure 1. Schematic of Clinical Sample Collection

Molecular and data analysis Protocol
- Genomic DNA from tumor/germline pairs (n=67) and cfDNA from 510 plasma samples were isolated.
- WGS of tumor/germline pairs followed by genome-wide integration of somatic mutations, enriched by signal processing and AI-based error suppression, were used to generate patient-specific tumor signature (Figure 2).
- Patient-specific somatic variants were used for detecting ctDNA levels in about 15 ng cfDNA from plasma WGS data by the MRDetect5 algorithm (Figure 2)
- Clinical data, such as pathological evaluation and radiographic imaging, were first unblinded after analysis and compared directly to the MRDetect5 plasma call results.
Figure 2. Schematic of Workflow

Figure 3. Concordance between independent laboratories - United States vs. Denmark

Figure 4. Prognostic value of circulating tumor DNA (ctDNA)

Kaplan-Meier survival analysis of recurrence-free survival (RFS)(A+B) and overall survival (OS) (C) stratified by ctDNA status before chemotherapy (or at diagnosis), before cystectomy, and any time after cystectomy.
(A) The follow-up time set to one year after last plasma sample fore each patient if prior to relapse, last CT scan or death.
(B+C) shows Kaplan-Meier analysis for the maximum follow-up time where patients without events were censored at end of follow-up.
Figure 5. Disease courses and longitudinal ctDNA results for the 67 patient study cohort
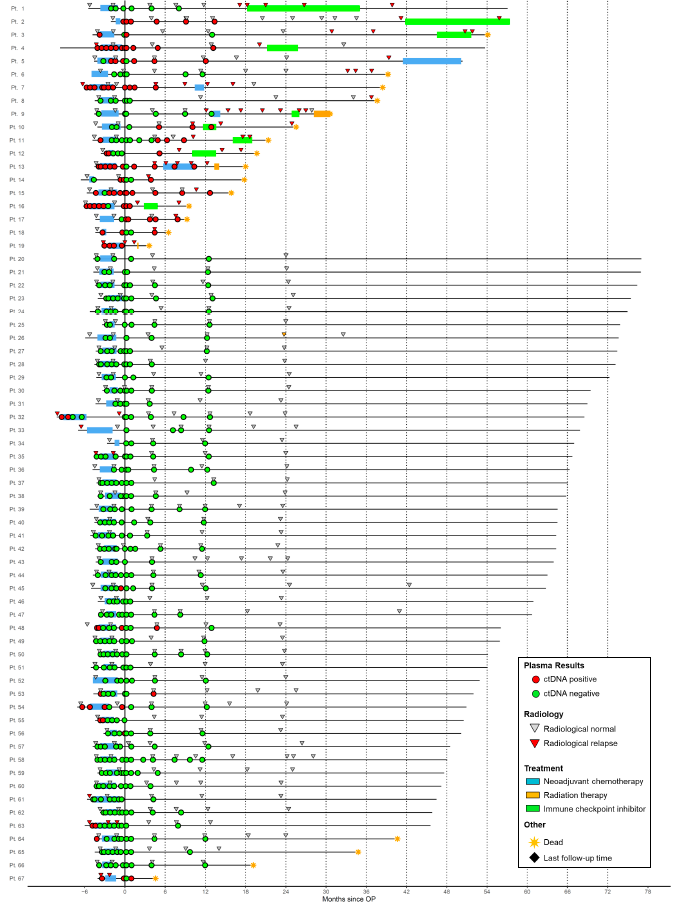
Longitudinal representation of ctDNA results and clinical parameters. Circles represent ctDNA status (see color code in the right box). Treatment and imaging information is indicated for each patient. Patients are separated into two groups on the basis of clinical relapse status. Metastatic relapse (Patient 1-19); Non Relapse (20-67).
Figure 6. Pathological downstaging vs. ctDNA status at diagnosis, pre-CX and post CX

Association between pathological downstaging and ctDNA status before chemotherapy, before cystectomy, and any time after cystectomy.
Figure 7. Prognostic value of circulating tumor DNA (ctDNA) detection - dichotomized analysis

Association between disease recurrence and ctDNA status before chemotherapy, before cystectomy, and any time after cystectomy.
Figure 8. Monitoring tumor fraction during patient disease courses

Figure 9. ctDNA dynamic during NAC as predictive markers of chemotherapy response
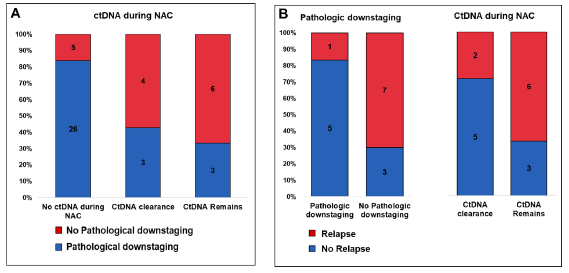
- (A) Association between ctDNA dynamic during NAC and pathological downstaging for ctDNA-negative patients (before and after NAC), patients where ctDNA was cleared during NAC, and patients in whom ctDNA remained
- (B) Association between recurrence and pathological downstaging (left) and ctDNA dynamics during NAC (right) for patients ctDNA-positive before NAC.
Figure 10. Lead time inferred from ctDNA-based recurrence detection

Lead time in days shown as the differences between first molecular relapse (ctDNA positive) and clinical recurrence (radiographic imaging positive). CT Scan corrected Lead time is calculated as the difference between the first CT scan after molecular relapse and clinical recurrence (see box in figure). The CT Scan corrected Lead time is more restrictive and included to provide a fair comparison to radiographic imaging.
Table 1. Patient Characteristics and Demographics (n=67)